Myalgic Encephalomyelitis/Chronic Fatigue Syndrome:An Endothelial–Neurovascular Hypothesis of Brainstem Oxygen Homeostasis Failure
- Graham Exelby
- Jul 5
- 4 min read

Dr Graham Exelby 2026
Abstract
Background: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a chronic multisystem disorder characterised by post-exertional malaise (PEM), autonomic dysfunction, cognitive impairment, sleep disturbance and profound loss of functional capacity. Although abnormalities involving cerebral perfusion, endothelial function, neurovascular coupling, mitochondrial metabolism, immune activation and autonomic regulation have each been described, these findings are generally considered in isolation and do not adequately explain the remarkable convergence of clinical features observed across patients with widely differing initiating events.
Hypothesis: We propose that failure of brainstem oxygen homeostasis represents the central physiological disturbance underlying ME/CFS. Within this framework, diverse initiating events—including viral infection, gastrointestinal disease, cervical trauma, connective tissue disorders, major surgery and sustained physiological stress—converge upon impaired oxygen delivery and utilisation within metabolically vulnerable brainstem nuclei. Progressive disruption of endothelial–pericyte function, neurovascular coupling, cerebral haemodynamics, mitochondrial oxidative metabolism and hypoxia-responsive signalling reduces the capacity to maintain integrated oxygen homeostasis.
Conceptual Framework: Failure of brainstem oxygen homeostasis initiates progressive depletion of physiological reserve across haemodynamic, autonomic, metabolic, inhibitory and inflammatory systems. Initially adaptive responses become maladaptive through persistent hypoxic signalling and neurovascular dysfunction, resulting in impaired physiological recovery. Within this model, post-exertional malaise represents the clinical manifestation of critically reduced physiological reserve rather than abnormal fatigue or isolated mitochondrial dysfunction.
Implications: This hypothesis integrates many previously competing biological models into a single physiological framework and generates testable predictions. It suggests that future research should focus on quantitative assessment of brainstem perfusion, neurovascular coupling, endothelial–pericyte function, cerebral oxygen utilisation, orthostatic haemodynamics and metabolic reserve. Therapeutic strategies aimed at restoring integrated brainstem oxygen homeostasis and rebuilding physiological reserve may provide a more effective approach than interventions directed at isolated downstream abnormalities.
Keywords: Myalgic encephalomyelitis; chronic fatigue syndrome; post-exertional malaise; brainstem; oxygen homeostasis; neurovascular coupling; endothelial dysfunction; pericytes; physiological reserve; hypoxia.
1. Introduction
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a chronic multisystem disease characterised by profound impairment in physical and cognitive function, autonomic dysfunction, sleep disturbance, sensory hypersensitivity and, most importantly, post-exertional malaise (PEM)—the delayed worsening of symptoms following physical, cognitive, orthostatic or emotional exertion.
Recognition of PEM as the defining clinical feature has fundamentally changed the understanding of the disease and now forms the cornerstone of contemporary diagnostic criteria, including the current UK National Institute for Health and Care Excellence (NICE) guideline (NG206). Rather than regarding fatigue as the principal abnormality, modern diagnostic frameworks recognise ME/CFS as a disorder of impaired physiological recovery, in which relatively minor physiological stressors may trigger prolonged deterioration lasting days or weeks.(1-4)
ME/CFS affects an estimated 0.2–0.8% of the population, although prevalence varies according to diagnostic criteria and case ascertainment. Women are affected approximately two to three times more frequently than men, and onset commonly follows an infectious illness, particularly infectious mononucleosis or, more recently, SARS-CoV-2 infection. However, a wide variety of other antecedent events have also been recognised, including gastrointestinal infections, major surgery, cervical trauma, connective tissue disorders and sustained physiological stress. The emergence of Long COVID has reinforced the concept that diverse initiating events may converge upon common downstream biological mechanisms rather than representing distinct disease entities.(5-8)
Over the past two decades, an increasingly consistent body of evidence has demonstrated that ME/CFS is associated with reproducible physiological abnormalities rather than a primary disorder of behaviour or motivation. Independent studies have identified cerebral hypoperfusion, abnormalities of brainstem structure and function, endothelial dysfunction, impaired oxygen extraction, autonomic dysregulation, altered cerebral blood flow regulation, mitochondrial dysfunction, inhibition of pyruvate dehydrogenase (PDH), characteristic metabolomic abnormalities, immune activation and neuroinflammation. Collectively, these observations support the concept of a disorder affecting integrated neurovascular and metabolic homeostasis rather than isolated dysfunction within a single organ system.(9-14)
Despite these advances, an important mechanistic question remains unresolved. Although cerebral and brainstem hypoperfusion have been repeatedly demonstrated, together with abnormalities of endothelial function, oxygen utilisation and mitochondrial metabolism, there is no widely accepted physiological framework that explains how these observations relate to one another or why patients with markedly different initiating illnesses ultimately develop a remarkably similar clinical syndrome. Current models frequently describe individual components of the disease but provide less explanation of how these diverse biological processes converge to produce the defining feature of ME/CFS—failure of recovery following physiological stress.(9,10, 12,13)
The brainstem represents a compelling candidate for this convergence. It integrates cardiovascular, respiratory, autonomic, metabolic and neuroimmune regulation through continuously active neuronal networks with exceptionally high metabolic demands. Unlike many cortical structures, these nuclei possess limited tolerance for sustained disturbances in oxygen homeostasis. Progressive impairment of oxygen delivery or utilisation within these metabolically vulnerable networks therefore has the potential to disrupt multiple homeostatic systems simultaneously while progressively reducing the physiological reserve required for recovery after exertion.(15-18)
This paper proposes an endothelial–neurovascular hypothesis in which diverse recognised initiating factors converge upon progressive failure of brainstem oxygen homeostasis. Rather than representing competing explanations, viral infection, immune dysregulation, gastrointestinal dysfunction, connective tissue disorders, endothelial injury, mechanical vascular abnormalities and other recognised contributors are interpreted as distinct pathways leading to a common physiological endpoint. Within this framework, persistent impairment of brainstem oxygen homeostasis initiates adaptive neurovascular and metabolic responses that progressively become maladaptive, culminating in depletion of physiological reserve and the emergence of post-exertional malaise as the clinical expression of impaired recovery.
Table 1. Established observations explained within the proposed framework.
Established observation | Proposed explanation within this hypothesis |
Brainstem hypoperfusion | Failure of regional oxygen homeostasis |
Cerebral hypoperfusion | Neurovascular dysregulation and impaired autoregulation |
PDH inhibition | Adaptive response to persistent hypoxia |
Low urinary aspartate | Declining metabolic reserve and impaired malate–aspartate shuttle |
Post-exertional malaise | Failure of physiological resolution after stress |
Progressive disability | Progressive depletion of integrated physiological reserve |
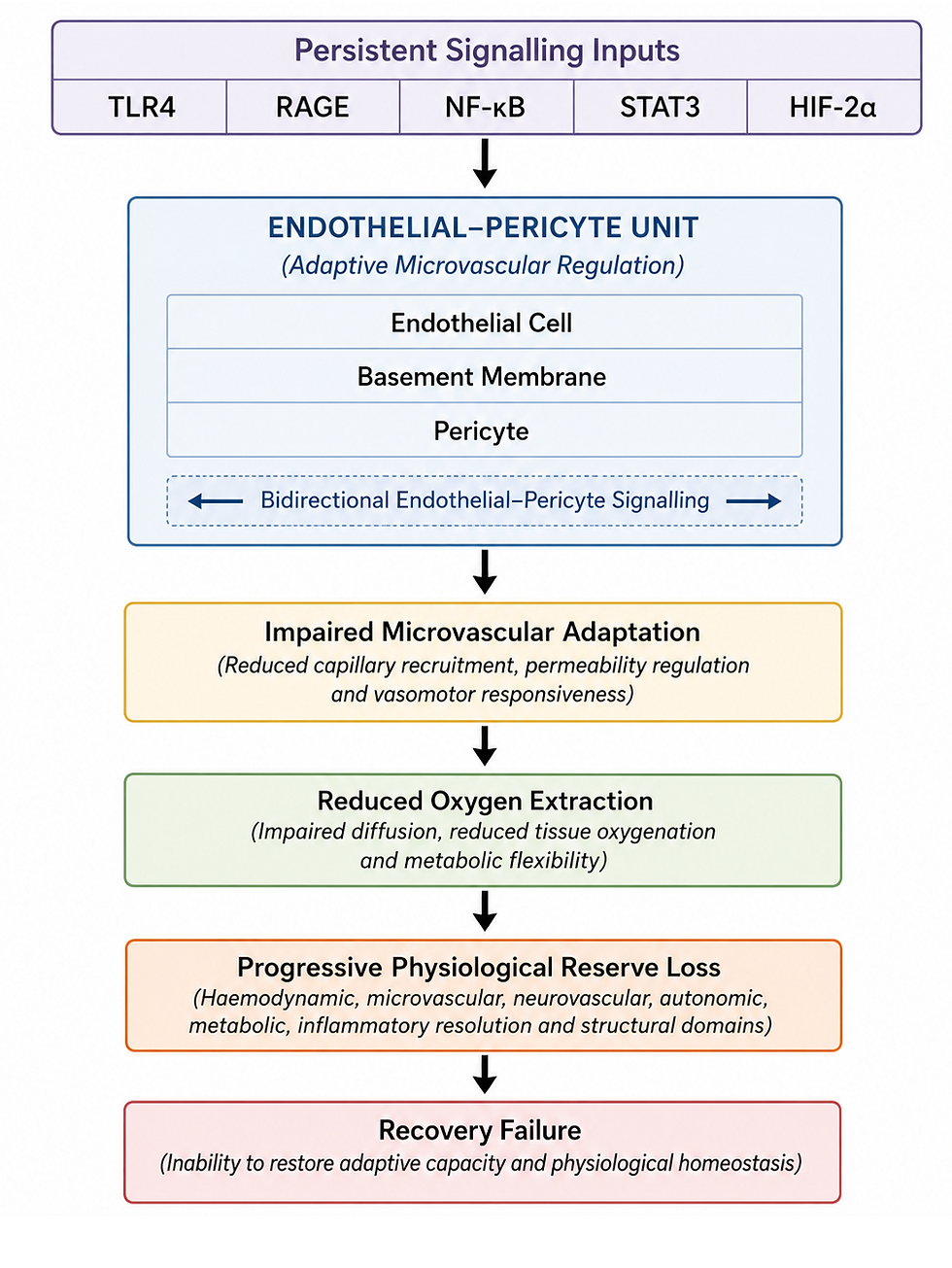
Within the proposed framework, persistent activation of interacting endothelial, inflammatory, neurovascular and hypoxia-responsive pathways—including RAGE, TLR4, maladaptive RAAS signalling, endothelial–pericyte dysfunction and chronic hypoxic adaptation—is proposed to converge upon a common physiological endpoint: failure of brainstem oxygen homeostasis. Progressive loss of integrated physiological reserve and post-exertional malaise are interpreted as the principal downstream clinical consequences of this convergence.
Full paper below.
Comments