A New Understanding of POTS, Long COVID and Related Disorders
- Graham Exelby
- Jun 13
- 5 min read

A personal update from Dr Graham Exelby June 2026
Over the past several years, what started as an attempt to better understand POTS has evolved into a much broader investigation of Long COVID, ME/CFS, Fibromyalgia, migraine, Ehlers-Danlos syndrome, chronic head pressure syndromes and related disorders.
The more patients we studied, the clearer it became that many of these conditions may not be separate diseases at all. Instead, they appear to share common physiological pathways involving autonomic dysfunction, preload failure, venous and lymphatic congestion, immune dysregulation, regional hypoxia, metabolic dysfunction and impaired tissue repair.
This website is currently undergoing major redevelopment.
Over 130 papers, reviews, clinical guides and patient resources are being prepared. These range from patient-friendly explanations through to GP resources and detailed scientific papers intended for specialists and researchers.
The work is taking longer than expected because the science continues to evolve.
Every month brings new findings that force us to rethink old assumptions.
The good news is that many of these findings are beginning to fit together.
Why I Started This Work
This work did not begin as a research project. It began with patients.
Many had been unwell for years. They had seen multiple specialists, undergone numerous investigations and often been told that everything was normal. Yet their symptoms persisted and, in many cases, continued to worsen.
As a clinician, it became increasingly difficult to ignore the recurring patterns. One patient would reveal part of the picture. The next would reveal another. Over time, the same themes appeared repeatedly, regardless of whether the diagnostic label was POTS, Long COVID, ME/CFS, migraine, Fibromyalgia or another related condition.
Each patient contributed another piece of a puzzle that gradually evolved into a different way of understanding these illnesses.
Where We Currently Believe the Field is Heading
Our current work suggests that many patients begin with a combination of genetic susceptibility and environmental triggers.
The genetic side frequently involves pathways regulating oxidative stress, immune signalling, inflammation, catecholamine metabolism and tissue repair. Variants involving COMT, TLR4, CCL2, STAT3, NF-κB and related pathways appear repeatedly.
Triggers may include:
• Viral infections, particularly COVID-19• Surgery and trauma• Concussion and neck injuries• Major physical or emotional stress• Pregnancy and hormonal change• Mould and environmental exposures• Connective tissue disorders
These triggers appear capable of initiating self-perpetuating cycles involving the immune system, blood vessels, lymphatics, nervous system and cellular energy production.
The Importance of Preload Failure
One of the most important observations from our clinic has been that many patients appear unable to maintain normal circulatory filling when upright.
This "preload failure" may arise from conditions such as:
• Thoracic Outlet Syndrome (TOS)• Nutcracker Syndrome• May-Thurner Syndrome• Pelvic Congestion Syndrome• Superior Mesenteric Artery Syndrome (SMA)• Azygous dysfunction and other venous abnormalities
These conditions are often missed because they cross traditional specialty boundaries.
Orthostatic echocardiography has demonstrated that many patients experience major reductions in stroke volume and cardiac output on standing, despite apparently normal conventional cardiac testing.
Head Pressure and Venous Congestion
Head pressure has emerged as one of the most useful clinical clues.
Some patients worsen primarily when upright.
Others worsen when lying down.
Many experience both.
Increasing evidence suggests that abnormalities of venous drainage, lymphatic clearance and cerebrospinal fluid dynamics may play important roles.
Particular attention has focused on internal jugular vein obstruction, upper cervical dysfunction, thoracic outlet pathology and impaired lymphatic drainage.
The Role of the Immune System
Perhaps the most exciting area of current research involves chronic immune activation.
Our attention has increasingly shifted toward interconnected pathways involving:
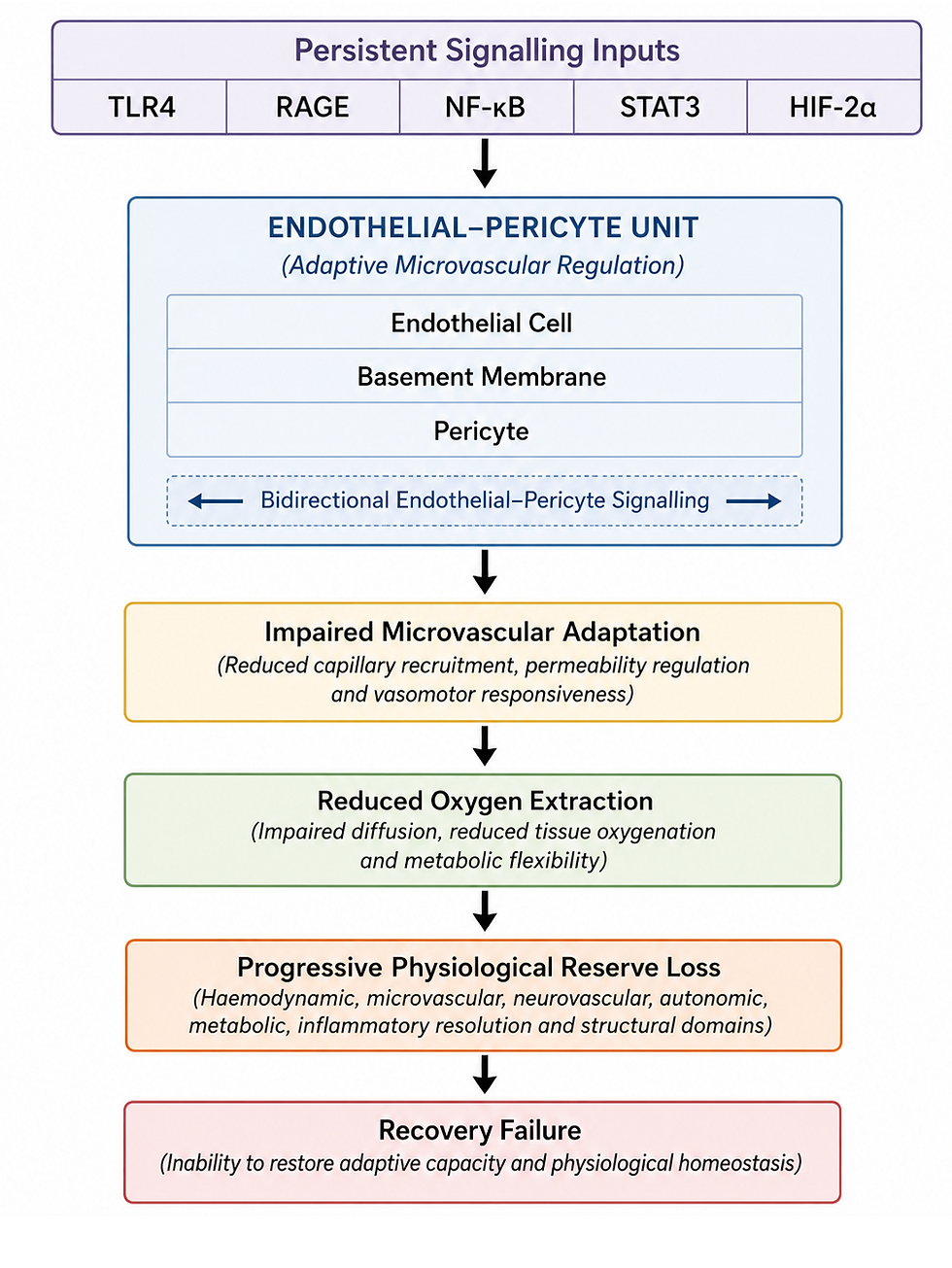
TLR4 → NF-κB → RAGE → STAT3 → CCL2
These pathways interact with mast cells, microglia, endothelial cells, pericytes and the extracellular matrix.
Once activated, they may continue to drive symptoms long after the original trigger has disappeared.
Understanding these pathways may ultimately explain why infections, trauma, mould exposure, surgery and other triggers can produce remarkably similar illnesses.
Pericytes and Regional Hypoxia
One area of particular interest is the role of the pericyte.
Pericytes help regulate blood flow at the microvascular level and sit at the intersection of vascular regulation, hypoxia sensing, inflammation and tissue repair.
Increasingly, we suspect that pericyte dysfunction may contribute to:
• RAAS dysregulation• Regional hypoxia• Brainstem dysfunction• Impaired tissue recovery• Progression from acute illness to chronic disease
This remains an evolving area of research but may prove to be one of the key missing pieces.
The Evolution of Disease
An important observation is that these illnesses appear to evolve over time.
The adolescent who develops early POTS following rapid growth, connective tissue vulnerability, SMA syndrome or thoracic outlet dysfunction is often very different from the patient presenting in their fifties or sixties with chronic inflammation, connective tissue remodelling, immune activation and vascular dysfunction.
Early disease often reflects physiological adaptation and compensation.
Later disease may involve structural changes, extracellular matrix remodelling, persistent inflammatory signalling, impaired tissue repair and progressive loss of physiological resilience.
Understanding where a patient sits along this continuum is often more important than the diagnostic label itself.
This concept is increasingly influencing how we investigate and manage patients.
Why Standard Tests Often Miss the Problem
Many patients are told that routine investigations are normal.
This does not mean nothing is wrong.
Most conventional tests are performed at rest and often fail to assess dynamic physiological function.
Our work increasingly relies on:
• Orthostatic echocardiography• Brain SPECT imaging• Dynamic vascular ultrasound• MRI venography• HRV and autonomic assessment• Amino acid profiling• Targeted physiological testing
These investigations frequently reveal abnormalities that are not visible on routine testing.
Recovery is Possible
Perhaps the most important lesson from this work is that improvement remains possible.
Patients frequently improve when the dominant physiological drivers are identified and addressed.
Treatment may involve combinations of:
• Autonomic stabilisation• Physical and manual therapies• Lymphatic therapies• Nutritional and metabolic support• Immune modulation• Management of venous compression syndromes• Targeted pharmacological interventions
No single treatment works for everyone.
The key is understanding which mechanisms are most important in each individual patient.
What Happens Next?
Over the coming months, this website will progressively be updated with:
• Patient education papers• GP clinical guides• Academic reviews• Research updates• Diagnostic frameworks• Treatment discussions• Case studies
The aim is simple: To provide a practical bridge between patients, clinicians and researchers.
If there is one message I hope visitors take away from this site, it is that these illnesses are not random and they are not imaginary.
The biology is complex, but increasingly understandable.
Every year we are learning more about the interactions between blood flow, immune signalling, autonomic function, metabolism, connective tissue, lymphatic function and recovery.
The goal of this work is not simply to explain disease. It is to identify practical pathways toward recovery, improved function and a better quality of life. Most importantly, to provide understanding, direction and hope.
Thank you for your patience while this work is being assembled.
Dr Graham Exelby
MCMC Research
Comments